
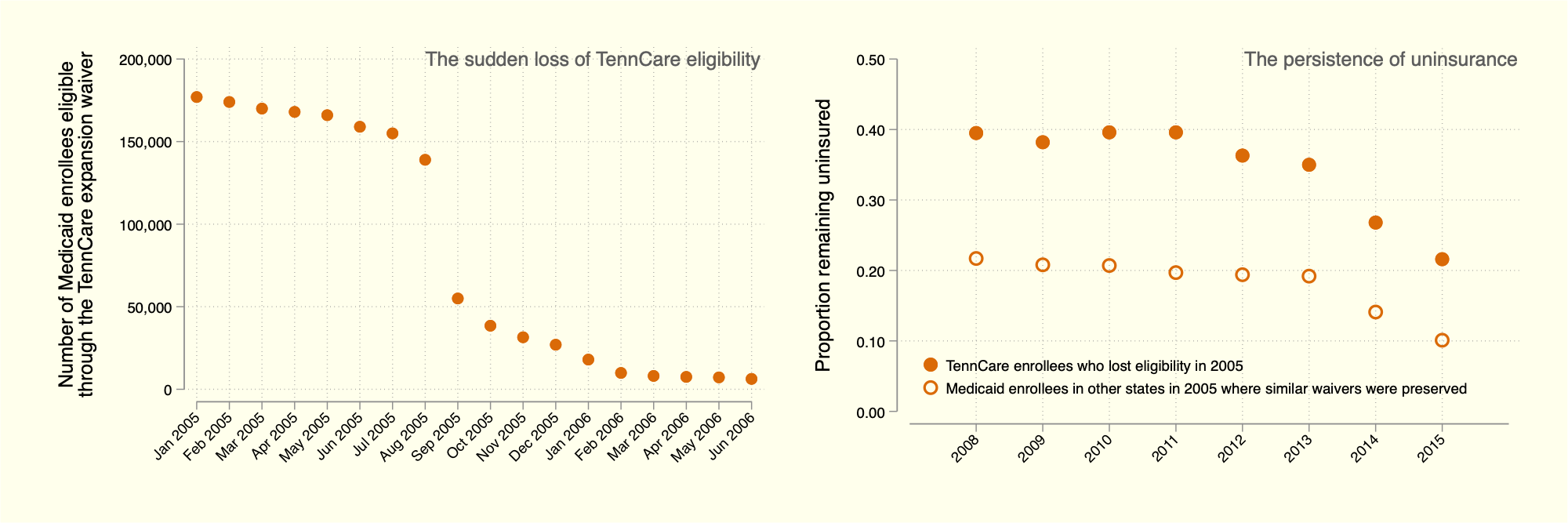
Above: We first illustrate the sudden cut to Medicaid eligibility among working-age adults in Tennessee in the middle of 2005. We then plot the fraction of (i) the “TennCare disenrollees” who remained uninsured many years after losing eligibility and (ii) adults enrolled in Medicaid in 2005 in states where similar waivers for eligibility remained intact.
Working paper temporarily unavailable
Abstract
Amid the largest rollback of Medicaid in generations, we study what was, at that time, the largest cut in US history, when the State of Tennessee suddenly and swiftly cut from its Medicaid rolls nearly four percent of the state’s working-age population. Although the “TennCare disenrollment” has been studied in the past, never has the set of disenrollees been identified and tracked over a long period of time, as we do in this paper by linking administrative enrollment records to large household surveys and to complete death records. We first show that nearly half of the approximately 170,000 TennCare disenrollees were still uninsured several years after the disenrollment. This is true despite 40,000 disenrollees getting back onto Medicaid rolls immediately through alternative bases of eligibility and despite 2,000 disenrollees aging onto Medicare each year. Although many disenrollees obtained insurance through an employer, we do not find increases in labor force participation or employment among the disenrolled. We do find, however, evidence that employees increased hours worked, ostensibly to qualify for health insurance with their employer. We also consider the health outcomes of the disenrollees, namely rates of disability and mortality. We find no evidence of an increase in either, whether soon or long after disenrollment, which puts our estimates more in the line with the experimental than the quasi-experimental literature on Medicaid and health. We caution that mortality effects are particularly difficult to detect, generally requiring large sample sizes, and we close by emphasizing that our “template” can be applied to study other changes in access to Medicaid, such as the cuts now underway for millions of low-income Americans.
Disclaimer: Any views expressed are those of the authors and not those of the U.S. Census Bureau. The Census Bureau has reviewed this data product to ensure appropriate access, use, and disclosure avoidance protection of the confidential source data used to produce this product. This research was performed at a Federal Statistical Research Data Center under FSRDC Project Number 2603. (CBDRB-FY21-P2603-R09240, CBDRB-FY25-P2603-R11872/12193)