
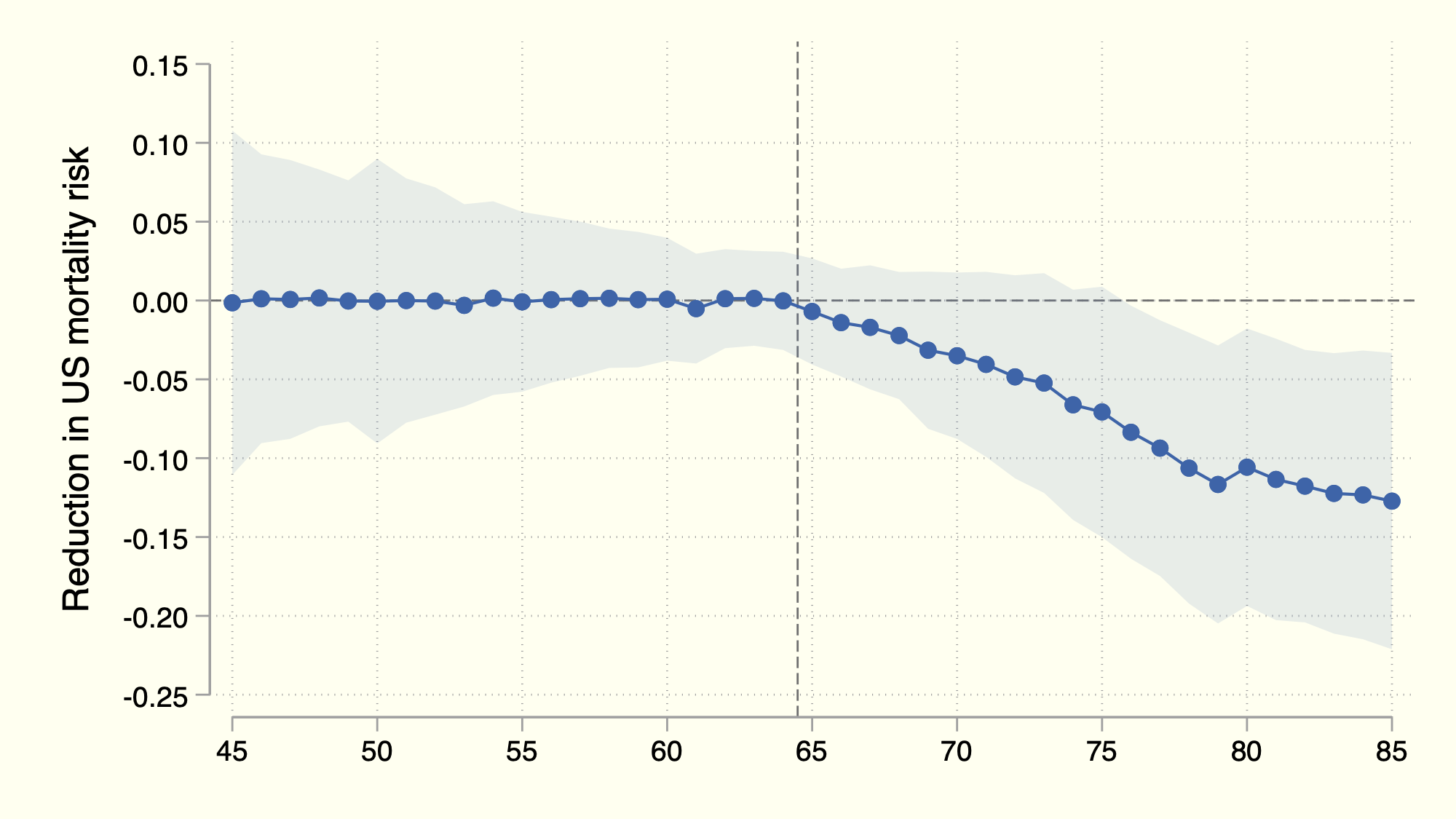
Above: We show that, as soon as Americans qualify for Medicare at age 65, their mortality rates drop sharply below those of their international peers. Focusing on the years 2000 through 2019, we plot the percentage gap in mortality between the US and a blend of countries chosen to match American mortality rates up to age 65.
Link to working paper
Abstract
Medicare was created to bring older Americans the “healing miracle of modern medicine.” Nonetheless, even six decades after its creation, the degree to which Medicare improves health and survival remains uncertain. Researchers have extensively studied the short-term impacts around the eligibility threshold of age 65, but the long-term effects that accrue slowly are not known. We address this open question by leveraging the fact that near-universal health-insurance coverage begins at age 65 in the United States—and only in the United States. Specifically, we estimate the impact of Medicare on mortality over long horizons using a synthetic-control approach, which generates a counterfactual from a blend of other countries that closely matches age-specific mortality rates in the United States up to age 65. Our results, illustrated by a sudden and persistent departure of the United States from that counterfactual at age 65, indicate that Medicare has extended life expectancy at age 65 throughout its history by about eight months on average. Critically, a similar impact is still seen today. The constituent causes of death point decisively toward medical care as the central mechanism. Gains arise almost solely from reductions in deaths considered amenable to timely and effective treatment. Our results imply that Medicare recoups a substantial portion of its trillion-dollar annual bill through previously unknown extensions in longevity. We conclude that lowering the age of Medicare eligibility would generate benefits exceeding the net costs to Americans.